


Figure 1
chest x-ray

Pericardial calcifications, right atrium dilation and pleural thickening.
Cardiovascular
Case TypeClinical Cases
Authors
Matthieu Garnier 1, MD; Marie Brasseur 1, MD; Jean-Nicolas Dacher 1,2, MD, PhD
17 years, male
A Black African migrant teenager reporting no medical history except malaria attacks was admitted to our hospital for dyspnea, increasing abdominal perimeter, and face and lower limbs oedema.
Cardiac auscultation found a systolic mitral murmur.
Blood tests revealed cholestasis without jaundice nor hepatic cytolysis, and a 0.6 G/L lymphopenia.
Chest radiograph (fig1) showed enlargement of the right aspect of the heart evocative of right atrial dilatation.
Pleural thickening was shown.
In projection of the heart and spine, a linear, calcified opacity was visible.
Transthoracic echocardiography found mitral insufficiency related to mitral valve prolapse, a dilated left atrium. Filling pressures were increased, so restrictive cardiopathy was suggested.
Abdominal ultrasound disclosed congestive liver and ascites.
Cardiac MRI was performed. The two atria and both vena cavas were dilated.
Cardiac ventricles were tubular-shaped. There was neither dilatation nor hypertrophy.
Septal dyskinesia with bouncing was shown arguing for ventricular decoupling (fig2).
Left ventricular ejection fraction was mildly altered but no segmental kinetics anomaly was found.
After gadolinium injection, we noticed pericardial enhancement.
Pericardium was mildly thickened.
Unenhanced chest CT scan (Fig3) highlighted pericardium thickening and multiple pericardial calcifications, predominating at the inferior atrioventricular groove. The diagnosis of constrictive chronic pericarditis (CCP) was made.
Constrictive chronic pericarditis is a rare and severe cause of heart failure. Its prevalence is estimated 0.5-2% of heart diseases.
Causes are multiple: tuberculosis is a classical etiology, especially in endemic regions but proving the disease is frequently problematic.
In western countries, viral, iatrogenic (mediastinal radiotherapy, pericardectomy), and idiopathic causes predominate.
Differential diagnosis with restrictive cardiopathy is challenging whereas distinguishing between these two diseases has a major therapeutic impact. Surgery (decortication) may be an option in case of CCP.
Chronic constrictive pericarditis is the consequence of an increased stiffness of the pericardium which becomes an inextensible shell, compromising the ventricular filling during diastole. It explains the frequency of abdominal symptoms with congestive liver and ascites. Pseudo cirrhosis can be misleading like in the present case.
Cardiac MRI is essential to differentiate between CCP and restrictive cardiopathy [1,2,3] as transthoracic echocardiography cannot show pericardial thickening (which was not major in our case).
Dynamic study in MRI is key examination for establishing the differential diagnosis:
In normal heart, the pressure in the left ventricle is higher than that in the right ventricle during the entire cardiac cycle. That is the reason why the interventricular septum is always bulging to the right.
In CCP, the right ventricle is an elective site of pericardial calcifications, and ventricles share a limited space: the right ventricle fills with high pressure during diastole, and pressures tend to equalize between the two ventricles: it is called ventricular interdependence.
A septal paradoxical movement can be observed during diastole called “septal bounce” [1]
This septal movement is increased by deep inspiration and predominates at the basis of the ventricles.
These septal anomalies are not found in case of restrictive cardiopathy.
CT nicely complements MRI in such situation, showing pericardial calcifications.
Right cardiac catheterization confirms constriction, showing a typical aspect of “Dip and plateau”, and an equalization of pulmonary and systemic pressures during diastole.
Despite its rareness, CCP should be thought of in the context of dyspnea with abdominal symptoms.
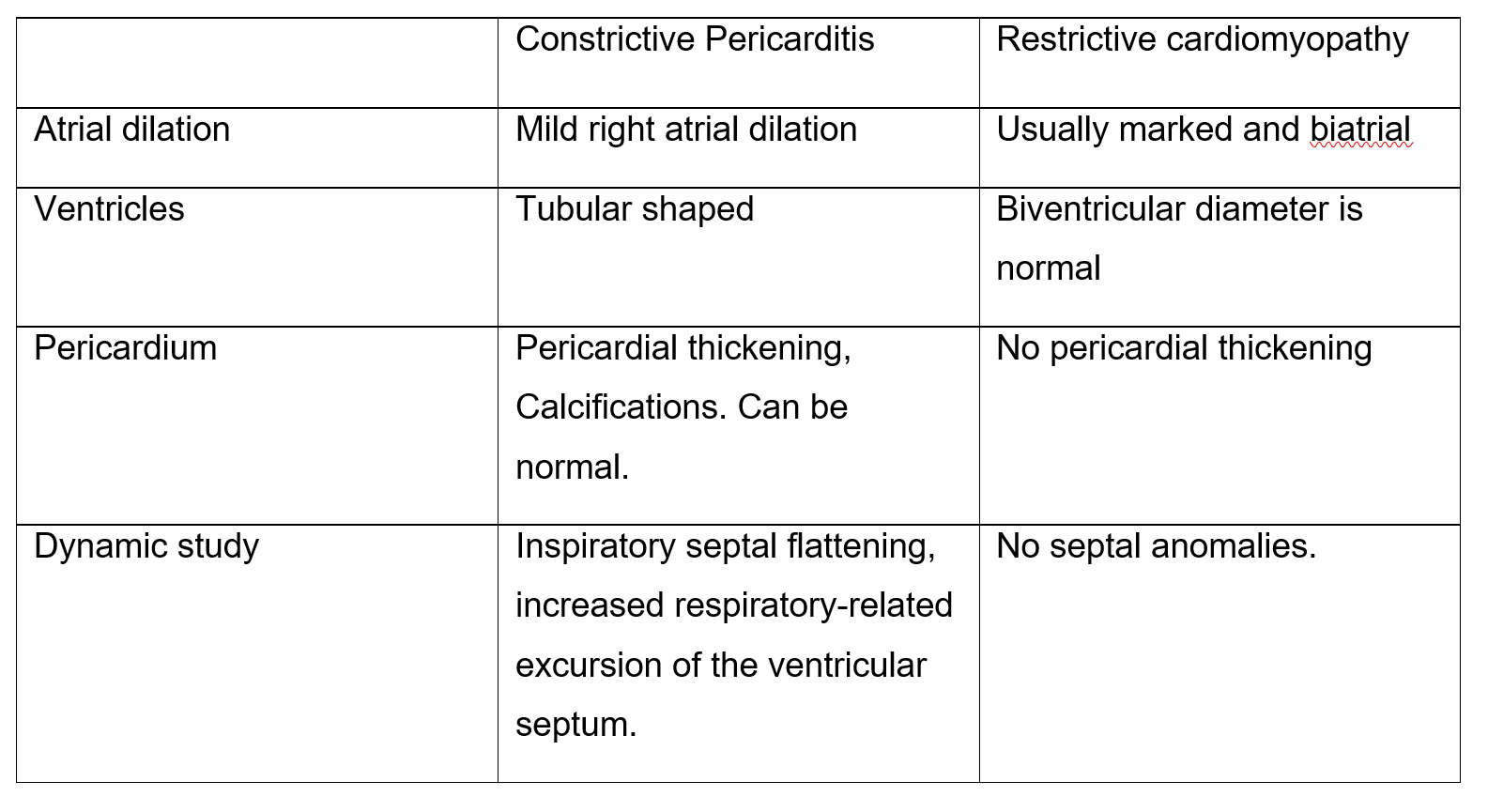
Table 1: Elements of differential diagnosis between constriction and restriction.
Written informed patient consent for publication has been obtained.
[1] Francone M, Dymarkowski S, Kalantzi M, Rademakers FE, Bogaert J. (2006) Assessment of ventricular coupling with real-time cine MRI and its value to differentiate constrictive pericarditis from restrictive cardiomyopathy. Eur Radiol. 2006 Apr;16(4):944-51. (PMID: 16228208)
[2] Bogaert J, Francone M. (2013) Pericardial disease: value of CT and MRI imaging.Radiology. 2013 May;267(2):340-56. (PMID: 23610095)
[3] Benedetta Giorgi , Nico R A Mollet, Steven Dymarkowski, Frank E Rademakers, Jan Bogaert (2003) Clinically Suspected Constrictive Pericarditis: MR Imaging Assessment of Ventricular Septal Motion and Configuration in Patients and Healthy Subjects Radiology. 2003 Aug;228(2):417-24. (PMID: 12802001)
| URL: | https://eurorad.org/case/16897 |
| DOI: | 10.35100/eurorad/case.16897 |
| ISSN: | 1563-4086 |
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.

chest x-ray
MRI video
CT scanner



