Clinical History
The patient was admitted to the hospital with sudden onset of left shoulder pain moving to the abdomen, presenting as an acute renal colic-like syndrome. There was no fever, no cough nor respiratory distress. She had no urinary complaints and didn't mention recent trauma. She had taken oral contraceptives for 14 years. Laboratory examinations revealed elevated CRP (7.2 mg/mL), proteinuria (0.24 g/h) and haematuria (urine-analysis: 76 RBC, 94% dysmorphic). Ultrasonography and CT scan were performed. Duplex ultrasonography was repeated after therapy.
Imaging Findings
A 33-year-old female was admitted to the hospital with sudden onset of left shoulder pain moving to the abdomen, presenting as an acute renal colic-like syndrome. There was no fever, no cough nor respiratory distress. She had no urinary complaints and didn't mention recent trauma. She had taken oral contraceptives for 14 years. Laboratory examinations revealed elevated CRP (7.2 mg/mL), proteinuria (0.24 g/h) and haematuria (urine-analysis: 76 RBC, 94% dysmorphic). Ultrasonography and CT scan were performed. Duplex ultrasonography was repeated after therapy.
The clinical data, with the pertinent predisposing factor of oral contraceptives and imaging findings are diagnostic for acute (partial) thrombosis of the renal vein.
Discussion
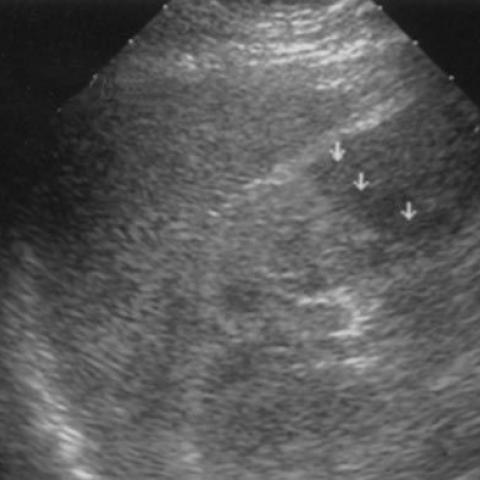
Increased renal size, altered echogenicity, loss of corticomedullary demarcation, enlargement of the renal vein and demonstration of a thrombus are indicative but non specific ultrasonographic findings of renal vein thrombosis. They may be entirely absent in equivocal cases.
Doppler analysis of the intrarenal arterial flow may demonstrate markedly reduce diastolic flow or inversed diastolic flow. This is suggestive for increased intrarenal pressure due to interstitial oedema and venous obstructive disease.
The diagnosis of partial renal vein thrombosis was suggested at ultrasonography and confirmed with contrast enhanced spiral CT which is much more appropriate. After thrombolytic treatment patency of the renal vein regained, as proven by disappearance of the thrombus on CT and the normal perfusion of the renal parenchyma at duplex ultrasonography.
Other acute diseases affecting one kidney that may cause asymmetric elevation of the resistive indices are ureteral stone and acute pyelonephritis. Patient's history is an important key in the differential diagnosis.
Differential Diagnosis List