Figure 1
Initial radiography

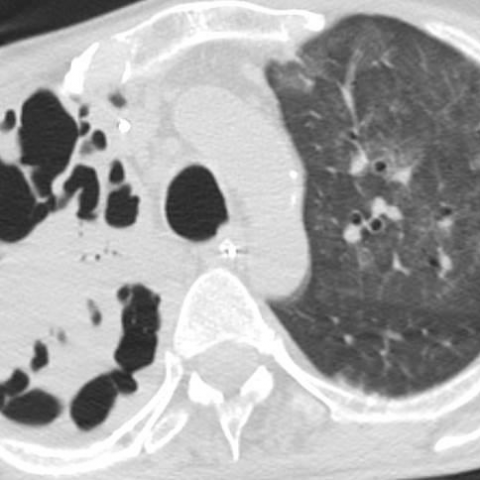
Extensive right upper lobe consolidation, with bulging of the horizontal fissure.
Chest imaging
Case TypeClinical Cases
AuthorsOchoa Y, Brugger S, Sopena P
52 years, male
[1] Holmes RB (1956) Friedlander’s pneumonia. Am J Roentgenol Radium Ther Nucl Med 75:728–47 (PMID: 13302536)
[2] Kang CI, Kim SH, Bang JW, Kim HB, Kim NJ, Kim EC, Oh MD, Choe KW (2006) Community-acquired versus nosocomial Klebsiella pneumoniae bacteremia: clinical features, treatment outcomes, and clinical implication of antimicrobial resistance. J Korean Med Sci 21(5):816-22 (PMID: 17043412)
[3] Tseng, C. P., Wu, H. S., Wu, T. H., Lin, Y. T., Fung, C. P (2013) Clinical characteristics and outcome of patients with community-onset Klebsiella pneumoniae bacteremia requiring intensive care. Journal of Microbiology, Immunology and Infection 46(3), 217-223 (PMID: 22832028)
[4] Okada F, Ando Y, Honda K. (2010) Acute Klebsiella pneumoniae pneumonia alone and with concurrent infection: comparison of clinical and thin-section CT findings. Br J Radiol 83 (994): 854-60 (PMID: 20647513)
[5] 5. Lim, W. S., Baudouin, S. V., George, R. C., Hill, A. T., Jamieson, C., Le Jeune, I., & Woodhead, M. A. (2009) BTS guidelines for the management of community acquired pneumonia in adults: update 2009. Thorax 64 (Suppl 3), iii1-iii55 (PMID: 19783532)
[6] Marshall GB, Farnquist BA, MacGregor JH, Burrowes PW (2006) Signs in Thoracic Imaging. J Thorac Imaging 21(1):76-90 (PMID: 16538167)
[7] Gadkowski LB, Stout JE (2008) Cavitary pulmonary disease. Clin. Microbiol. Rev 21(2):305-33 (PMID: 18400799)
[8] Okada F, Ando Y, Honda K, Nakayama T, Kiyonaga M, Ono A, Tanoue S, Maeda T, Mori H (2009) Clinical and pulmonary thin-section CT findings in acute Klebsiella pneumoniae pneumonia. Eur Radiol 19(4):809-15 (PMID: 19034459)
[9] Moon, W. K., Im, J. G., Yeon, K. M., & Han, M. C (1995) Complications of Klebsiella pneumonia: CT evaluation. J Comput Assist Tomogr 19(2):176-181 (PMID: 7890837)
[10] Pande, A., Nasir, S., Rueda, A. M., Matejowsky, R., Ramos, J., Doshi, S., & Musher, D. M. (2011) The Incidence of Necrotizing Changes in Adults With Pneumococcal Pneumonia. Clinical infectious disease cir749 (PMID: 22042878)
[11] Löffler B, Niemann S, Ehrhardt C, Horn D, Lanckohr C, Lina G, Ludwig S, Peters G. (2013) Pathogenesis of Staphylococcus aureus necrotizing pneumonia: the role of PVL and an influenza coinfection. Expert Rev Anti Infect Ther 11(10):1041-51 (PMID: 24073746)
[12] Vayalumkal JV, Whittingham H, Vanderkooi O, Stewart TE, Low DE, Mulvey M, McGeer A. (2007) Necrotizing pneumonia and septic shock: suspecting CA-MRSA in patients presenting to Canadian emergency departments. CJEM 9(4):300-3. (PMID: 17626697)
| URL: | https://eurorad.org/case/12729 |
| DOI: | 10.1594/EURORAD/CASE.12729 |
| ISSN: | 1563-4086 |
Initial radiography
Chest CT
Chest radiograph 2 weeks later
Chest CT 2 weeks later