Figure 1
Shoulder X-ray

Shoulder soft tissue swelling and erosion of the distal clavicle.
Musculoskeletal system
Case TypeClinical Cases
AuthorsRaquel Monreal Beortegui, Jokin Zabalza Unzué, Ainhoa Ovelar Ferrero, Nerea Baraibar Argota.
69 years, female
[1] Gabriel SE. (2001) The epidemiology of rheumatoid arthritis. Rheum Dis Clin North Am 27(2):269-81 (PMID: 11396092)
[2] Wasserman AM. (2011) Diagnosis and management of rheumatoid arthritis. Am Fam Physician 84(11):1245-52 (PMID: 22150658)
[3] Grassi W, De Angelis R, Lamanna G, Cervini C. (1988) The clinical features of rheumatoid arthritis. Eur J Radiol 27 Suppl 1:S18-24. (PMID: 9652497)
[4] Andrew L. Chen, Thomas N. Joseph, Joseph D. Zuckerman (2003) Rheumatoid Arthritis of the Shoulder. J Am Acad Orthop Surg 11(1):12-24. (PMID: 12699368)
[5] Bodolay E, Koch AE, Kim J, Szegedi G, Szekanecz Z. (2002) Angiogenesis and chemokines in rheumatoid arthritis and other systemic inflammatory rheumatic diseases. J Cell Mol Med 6(3):357-76. (PMID: 12417052)
[6] Vasanth LC, Pavlov H, Bykerk V. (2013) Imaging of rheumatoid arthritis. Rheum Dis Clin North Am 139(3):547-66 (PMID: 23719075)
[7] Resnick D, Niwayama G. (1976) Resorption of the undersurface of the distal clavicle in rheumatoid arthritis. Radiology 120(1):75-7. (PMID: 935467)
[8] Sussmann AR, Cohen J, Nomikos GC, Schweitzer ME. (2012) Magnetic resonance imaging of shoulder arthropathies. Magn Reson Imaging Clin N Am 20(2):349-71 (PMID: 22469408)
[9] Sommer OJ, Kladosek A, Weiler V, Czembirek H, Boeck M, Stiskal M. (2005) Rheumatoid arthritis: a practical guide to state-of-the-art imaging, image interpretation, and clinical implications. Radiographics 25(2):381-98 (PMID: 15798057)
[10] Schoellnast H, Deutschmann HA, Hermann J, Schaffler GJ, Reittner P, Kammerhuber F, Szolar DH, Preidler KW. (2006) Psoriatic arthritis and rheumatoid arthritis: findings in contrast-enhanced MRI. AJR Am J Roentgenol 187(2):351-7 (PMID: 16861537)
[11] Narváez JA, Narváez J, De Lama E, De Albert M. (2010) MR imaging of early rheumatoid arthritis. Radiographics 30(1):143-63 (PMID: 20083591)
[12] Narváez JA, Narváez J, Roca Y, Aguilera C. (2002) MR imaging assessment of clinical problems in rheumatoid arthritis. Eur Radiol 12(7):1819-28 (PMID: 12111074)
[13] Popert AJ, Scott DL, Wainwright AC, Walton KW, Williamson N, Chapman JH. (1982) Frequency of occurrence, mode of development, and significance or rice bodies in rheumatoid joints. Ann Rheum Dis 41(2):109-17. (PMID: 6176192)
| URL: | https://eurorad.org/case/14322 |
| DOI: | 10.1594/EURORAD/CASE.14322 |
| ISSN: | 1563-4086 |
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.

Shoulder X-ray
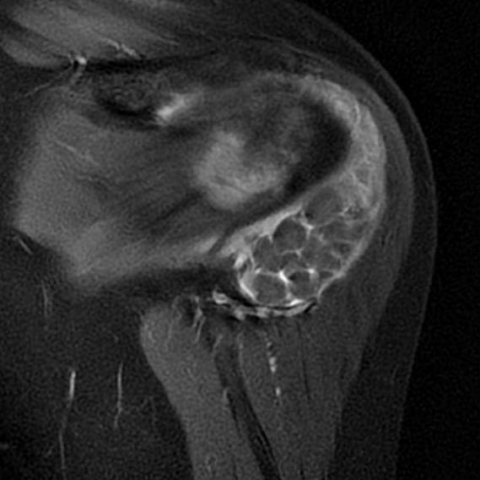
Coronal MRI images
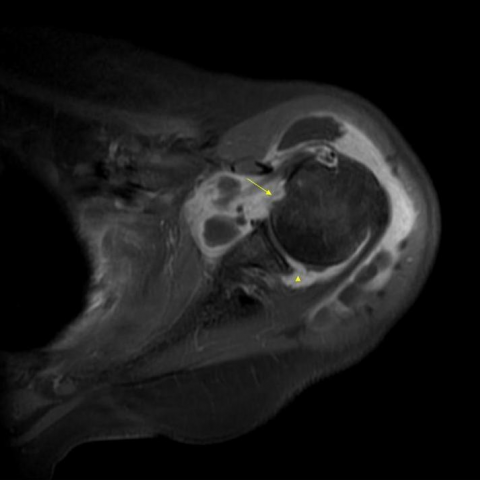
Coronal and axial T1-weighted fat saturated post gadolinium images
Gradient-echo sequence