Figure 1
MRI - Precontrast images

Axial (a), detail coronal (b) and sagittal (c) T2-weighted images showed complex abdominal wall mass including a central portion (*) with heterogeneous signal, surrounded by several cyst-like structures, the largest with fluid-fluid level (arrowhead).

Detail T2-weighted images showed a complex, lobulated abdominal wall mass including a central portion (*) with heterogeneous intermediate-to-high signal, surrounded by several cyst-like structures.

Detail T2-weighted images showed a lobulated mass including a central portion (*), surrounded by several cyst-like structures. Note infiltration of rectus abdominis muscle, linear bands (thin arrows) radiating into the surrounding fat.

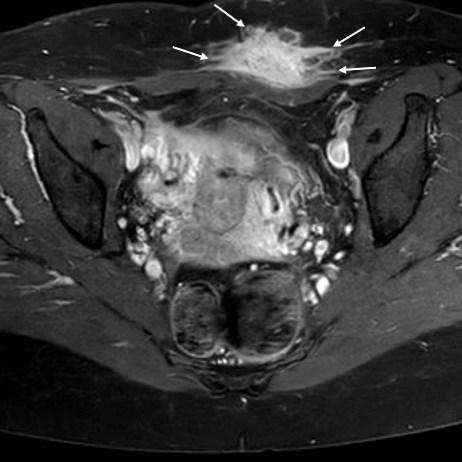
Fat-suppressed T2-weighted images confirmed complex, abdominal wall mass including a central portion (*) and peripheral cyst-like structures, linear bands (thin arrows) radiating into the surrounding fat.

Fat-suppressed T1-weighted images confirmed complex abdominal wall mass including a solid central portion (*) and peripheral cyst-like structures with T1 hyperintensity indicating recent blood and fluid-fluid level (arrowhead).