


Figure 1
Hyperdense cholesteatoma of the external auditory canal: an unusual appearance of a common lesion in an uncommon location
SectionHead & neck imaging
Case TypeClinical Cases
Authors
Dr. Naufal P, Dr. Athira Prasad, Dr. Devarajan E, Dr. Saanida MP, Dr. Juvaina P, Dr. John J Nalappat
Connected authors
64 years, female
Clinical History
A 64-year-old female with recurrent episodes of left-sided earache, otorrhea and hearing defect for past four years; now with worsening of symptoms accompanied by giddiness, vomiting and facial deviation to right for one month. There is history of trauma to the external ear four years back.
Imaging Findings
High resolution computed tomography (plain and contrast) of the temporal bone was done. A well-defined homogenously hyperdense lesion of average Hounsfield units 170 was noted in the external auditory canal with extension into the middle ear and mastoid cavities. No significant enhancement was noted on post contrast images. The lesion was noted to cause blunting of the scutum and erosion of the anterior and posterior walls of external auditory canal, mastoid walls and tympanic segment of the facial canal. Erosion of body, long and short processes of incus was also noted.
Based on the computed tomography findings of a non-enhancing lesion in the external auditory canal with extension into middle ear and mastoid cavity and bony erosion, a probable diagnosis of cholesteatoma was made. Imaging differentials of keratosis obturans and mycetoma was also kept.
Mastoid exploration was done and the histopathology proved it to be cholesteatoma.
Discussion
Cholesteatomas occur due to the ingrowth of the stratified squamous epithelium of the external auditory canal into the middle ear. External auditory canal cholesteatomas are rare occurring in about 1-5 of every 1000 otologic cases [1]. Most of the cases are spontaneous but can occur secondary to trauma or surgery. [2].
Usual symptoms include otalgia, otorrhea and hearing loss [3].
Cholesteatoma of the external auditory canal appears as a soft tissue attenuating lesion with bone erosion and with intramural bone fragments [4]. However, a homogenously hyperdense appearance is not described which is peculiar to our case.
According to the clinical and computed tomography staging by Seung-Ho Shin et al there are four groups of external auditory canal cholesteatoma [5]. In stage I, the disease limited to the external auditory canal. There is involvement of tympanic membrane and middle ear in stage II. In stage III there is involvement of mastoid air cells. There is extension beyond the temporal bone in stage IV. The case under discussion is in stage III.
The management of the external auditory canal cholesteatoma depends on the extent of the lesion. In case of involvement of the mastoid air cells as in our case, the appropriate procedure should be canaloplasty with mastoidectomy [5].
An external auditory canal cholesteatoma can be mimicked by many conditions like keratosis obturans, carcinoma etc, computed tomographic imaging of the temporal bone is useful in arriving at the correct diagnosis, to determine the extent of the lesion and the bony involvement.
Our patient had a previous history of trauma which could be the inciting event for the secondary cholesteatoma formation. The features of facial palsy alerted the ENT surgeon to a pathology not confined to the external auditory canal but extending to the middle ear.
The imaging differentials include keratosis obturans and mycetoma. Keratosis obturans is the pathological condition characterised by accumulation of desquamated keratin in the external auditory meatus. The features which made keratosis obturans less likely was the chronic history and the irregular bony erosions instead of the smooth scalloping seen in keratosis. Mycetoma of the mastoid with bony erosions are described, but extensive disease with ossicular erosions are not reported.
To conclude, external auditory canal cholesteatoma can have atypical imaging appearances as hyperdense lesions with high HU values. A confident diagnosis in such scenarios is aided by the presence of accompanying bone destruction and absent contrast enhancement.
Differential Diagnosis List
Spontaneous hyperdense cholesteatoma of the external auditory canal
Cholesteatoma
Keratosis obturans
Mycetoma
Final Diagnosis
Spontaneous hyperdense cholesteatoma of the external auditory canal
References
[1] Anthony PF, Anthony WP. Surgical treatment of external auditory canal cholesteatoma. Laryngoscope 1982;92:70–75 (PMID: 7162301)
[2] Holt JJ. Ear canal cholesteatoma. Laryngoscope 1992;102:608–613 (PMID: 1376388)
[3] Tran LP, Grundfast KM, Selesnick SH. Benign lesions of the external auditory canal. Otolaryngol Clin North Am 1996;29:807–825 (PMID: 8893218)
[4] Heilbrun ME, Salzman KL, Glastonbury CM, Harnsberger HR, Kennedy RJ, Shelton C. External auditory canal cholesteatoma: Clinical and imaging spectrum. AJNR Am J Neuroradiol 2003;24:751‑6 (PMID: 12695217)
[5] Shin SH, Shim JH, Lee HK. Classification of External Auditory Canal Cholesteatoma by Computed Tomography. Clini Experimental Otorhinolaryngol 2010;3:24-6 (PMID: 20379398)
Case information
| URL: | https://eurorad.org/case/17326 |
| DOI: | 10.35100/eurorad/case.17326 |
| ISSN: | 1563-4086 |
License
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.



Figure 2

coronal CT sections showing the lesion with involvement of external auditory canal, middle ear and mastoid
Figure 3

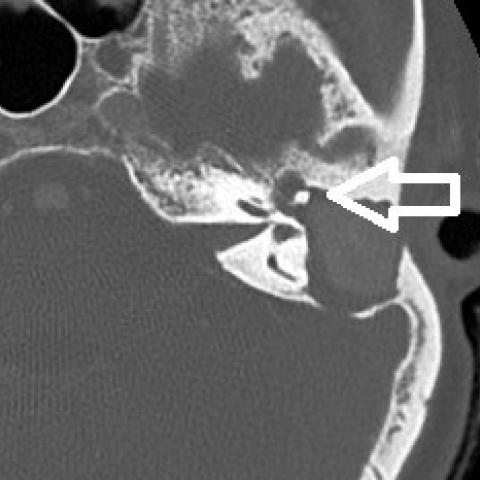
axial CT sections showing bony erosion of external auditory canal(a), ossicular chain(b), mastoid(c) and tympanic segment of facial canal(d)
axial CT sections showing bony erosion of external auditory canal(a), ossicular chain(b), mastoid(c) and tympanic segment of facial canal(d)

axial CT sections showing bony erosion of external auditory canal(a), ossicular chain(b), mastoid(c) and tympanic segment of facial canal(d)

axial CT sections showing bony erosion of external auditory canal(a), ossicular chain(b), mastoid(c) and tympanic segment of facial canal(d)



axial CT sections showing hyperdense lesion in the mastoid in plain (a) and with no significant enhancement on post contrast images (b)
Department of Radiodiagnosis, Government Medical College, Kozhikode, Kerala, India, 2020
Department of Radiodiagnosis, Government Medical College, Kozhikode, Kerala, India, 2020

axial CT sections showing hyperdense lesion in the mastoid in plain (a) and with no significant enhancement on post contrast images (b)
Department of Radiodiagnosis, Government Medical College, Kozhikode, Kerala, India, 2020
Department of Radiodiagnosis, Government Medical College, Kozhikode, Kerala, India, 2020

coronal CT sections showing the lesion with involvement of external auditory canal, middle ear and mastoid
Department of Radiodiagnosis, Government Medical College, Kozhikode, Kerala, India, 2020
Department of Radiodiagnosis, Government Medical College, Kozhikode, Kerala, India, 2020

axial CT sections showing bony erosion of external auditory canal(a), ossicular chain(b), mastoid(c) and tympanic segment of facial canal(d)
Department of Radiodiagnosis, Government Medical College, Kozhikode, Kerala, India, 2020
Department of Radiodiagnosis, Government Medical College, Kozhikode, Kerala, India, 2020

axial CT sections showing bony erosion of external auditory canal(a), ossicular chain(b), mastoid(c) and tympanic segment of facial canal(d)
Department of Radiodiagnosis, Government Medical College, Kozhikode, Kerala, India, 2020
Department of Radiodiagnosis, Government Medical College, Kozhikode, Kerala, India, 2020

axial CT sections showing bony erosion of external auditory canal(a), ossicular chain(b), mastoid(c) and tympanic segment of facial canal(d)
Department of Radiodiagnosis, Government Medical College, Kozhikode, Kerala, India, 2020
Department of Radiodiagnosis, Government Medical College, Kozhikode, Kerala, India, 2020

axial CT sections showing bony erosion of external auditory canal(a), ossicular chain(b), mastoid(c) and tympanic segment of facial canal(d)
Department of Radiodiagnosis, Government Medical College, Kozhikode, Kerala, India, 2020
Department of Radiodiagnosis, Government Medical College, Kozhikode, Kerala, India, 2020

200X biopsy sections showing stratified squamous epithelium (white arrow), keratin debris (black arrow) and a few chronic inflammatory cells
Department of Radiodiagnosis, Government Medical College, Kozhikode, Kerala, India, 2020
Department of Radiodiagnosis, Government Medical College, Kozhikode, Kerala, India, 2020

200X biopsy sections showing stratified squamous epithelium (white arrow), keratin debris (black arrow) and a few chronic inflammatory cells
Department of Pathology, Government Medical College, Kozhikode, Kerala, India, 2020
Department of Pathology, Government Medical College, Kozhikode, Kerala, India, 2020