


Figure 1
Teaching Case
SectionBreast imaging
Case TypeClinical Cases
Authors
Erkin Aribal
Connected authors
62 years, female
A 62-year-old healthy woman presents with a retroareolar lump in the right breast. The mass was painless and the patient did not have any physical findings other than the right breast lump.
Primary diffuse large B cell lymphoma of the breast
Primary breast lymphoma
Triple Negative invasive cancers of the breast
Mucinous cancer of the breast
Phyllodes tumour
Papillary carcinoma of the breast
The mammogram shows a retroareolar mass of 3cm in diameter (fig. 1). The mass is dense, round and shows circumscribed margins (fig. 1). The ultrasound findings show a hypoechoic oval mass with microlobular margins and show slight posterior enhancement. On Doppler imaging, the vascularity of the tumour is not well seen (fig. 2B), but microvascular imaging shows vessels inside the mass (fig 2C). On MRI, the mass is round with irregular margins, isoechoic in T1 weighted images, and hyperechoic in T2 weighted STIR images (Fig 3A, B). Dynamic contrast-enhanced images show a type 3 almost homogenous contrast enhancement with an early initial high uptake and late washout (Fig 3C,D). The diffusion-weighted images show diffusion restriction with an ADC value at 0,680x10-3 mm2/s (Fig 3E,F). PET imaging shows high FDG uptake of the lesion (Fig 4).
Ultrasound-guided core needle biopsy of the lesion showed diffuse large B cell lymphoma of the breast. PET imaging did not show any FDG uptake other than the mass in the right breast.
Breast lymphoma constitutes 0.04%–0.5% of all breast malignancies. It is less likely to be a primary lymphoma of the breast or can be a secondary breast lymphoma in cases with systemic involvement [1]. Primary breast lymphoma is frequently seen in women and manifests early in the sixth decade [1-3]. The majority of the cases are diffuse large B-cell lymphoma consisting of 45-79% of the cases, followed by follicular lymphoma, mucosa-associated lymphoid tissue lymphoma, and Burkitt lymphoma [1-4]. Primary lymphoma is usually presented unilaterally and predominantly seen in the right breast. Primary breast lymphoma usually presents with a painless enlarging mass and may show local inflammatory changes such as oedema and erythema, particularly in high-grade cases. However, retraction of the nipple or bloody discharge is uncommon [3-5].
Radiologic Findings
Mammography
At mammography, the typical findings of breast lymphoma are round or oval in shape with high density and commonly circumscribed margins. Although the margins can be indistinct, a spiculated margin is uncommon. Calcifications are not seen in or around the lesions. Associating findings such as skin thickening, edema, architectural distortion, or asymmetries are rarely defined. [6–8].
Ultrasonography
Primary lymphoma of the breast appears as an oval or irregular mass with circumscribed or non-circumscribed margins. Although ultrasound features are not specific, an oval hypoechoic circumscribed mass with a parallel orientation should raise suspicion for a lymphoma, particularly in women in the 6th decade (8,9). However, the internal echo pattern may show mixed echogenicity, and these masses are frequently hypervascular at Doppler ultrasound and may show a posterior acoustic enhancement [8-10].
MRI
At MRI, lymphomas show a mass with a round or oval shape, and the internal structure depicts hypo or isointense on T1 weighted images and slightly hyperintensity on T2 weighted images [9,11]. The margins can be circumscribed or irregular and may show spiculations [8]. It is reported that high-resolution images may show more irregular margins (8,9), and grossly circumscribed margins may have a spot of irregularity [8]. On dynamic contrast-enhanced series, these tumours frequently show homogeneous or mildly heterogeneous contrast enhancement, and rim enhancement is uncommon [6,8,9]. The kinetic enhancement pattern shows a rapid initial enhancement with a plateau in delayed phase or, less frequently, a washout pattern [6,11,12]. Adjacent vessel sign is a frequent finding [13]. Skin thickening and diffuse infiltration can be seen but a less common finding. MRI examination is important in defining the extent and multicentricity of the tumour. However, primary breast lymphoma is more often presented with a palpable solitary mass, and secondary lymphomas are more frequently detected as multicentric [6]. At diffusion-weighted images, the ADC values show lower than 0.9×10-3 mm2/s [8].
FDG PET Imaging
FDG PET shows high uptake of FDG in primary breast lymphoma and has a high sensitivity and specificity in detecting the extension of the lesion and monitoring the response to treatment [14].
References
[1] Jeanneret-Sozzi W, Taghian A, Epelbaum R, et al. Primary breast lymphoma: patient profile, out- come and prognostic factors. A multicentre Rare Cancer Network study. BMC Cancer 2008; 8:86.
[2] Broga E, Harris NL. Lymphomas of the breast: pathology and clinical behavior. Semin Oncol 1999;26(3):357–364
[3] Ryan G, Martinelli G, Kuper-Hommel M, et al. Primary diffuse large B-cell lymphoma of the breast: prognostic factors and outcomes of a study by the International Extranodal Lymphoma Study Group. Ann Oncol 2008;19(2):233–241.
[4] Gupta V, Bhutani N, Singh S, Chhabra S, Sen R. Primary non-Hodgkin’s lymphoma of breast: a rare cause of breast lump. Hum Pathol Case Rep 2017;7:47–50.
[5] Kuper-Hommel MJ, Snijder S, Janssen-Heijnen ML, et al. Treatment and survival of 38 female breast lymphomas: a population-based study with clinical and pathological reviews. Ann Hematol 2003;82(7):397–404.
[6] Yang WT, Lane DL, Le-Petross HT, Abruzzo LV, Macapinlac HA. Breast lymphoma: imaging findings of 32 tumors in 27 patients. Radiology 2007;245(3):692–702.
[7] Liberman L, Giess CS, Dershaw DD, Louie DC, Deutch BM. Non-Hodgkin lymphoma of the breast: imaging characteristics and correlation with histopathologic findings. Radiology 1994;192:157–160.
[8] Wang L, Wang D, Chai W, Fei X, Luo R, Li X. MRI features of breast lymphoma: preliminary experience in seven cases. Diagn Interv Radiol. 2015;21(6):441-7.
[9] Surov A, Holzhausen HJ, Wienke A, et al. Primary and secondary breast lymphoma: prevalence, clinical signs and radiological features. Br J Radiol 2012;85(1014):e195–e205.
[10] Irshad A, Ackerman SJ, Pope TL, Moses CK, Rumboldt T, Panzegrau B. Rare breast lesions: correlation of imaging and histologic features with WHO classification. RadioGraphics 2008;28(5):1399–1414.
[11] Liu K, Xie P, Peng W, Zhou Z. The features of breast lymphoma on MRI. Br J Radiol 2013; 86:20130220.
[12] Rizzo S, Preda L, Villa G, et al. Magnetic resonance imaging of primary breast lymphoma. Radiol Med (Torino) 2009;114(6):915–924.
[13] Dietzel M, Baltzer PA, Vag T, et al. The adjacent vessel sign on breast MRI: new data and a subgroup analysis for 1,084 histologically verified cases. Korean J Radiol 2010; 11:178–186.
[14] Santra A, Kumar R, Reddy R, et al. FDG PET-CT in the management of primary breast lymphoma. Clin Nucl Med 2009;34(12):848–853.
Case information
| URL: | https://eurorad.org/case/18035 |
| DOI: | 10.35100/eurorad/case.18035 |
| ISSN: | 1563-4086 |
License
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.



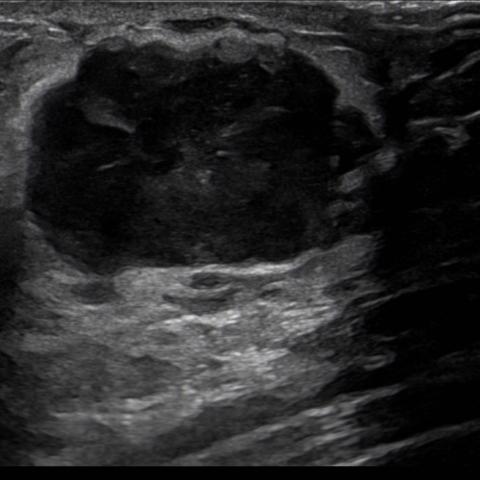














Figure 3

Breast Imaging Clinic, Acibadem Altunizade Hospital, Istanbul, Turkey, 2022

Breast Imaging Clinic, Acibadem Altunizade Hospital, Istanbul, Turkey, 2022

Breast Imaging Clinic, Acibadem Altunizade Hospital, Istanbul, Turkey, 2022

Breast Imaging Clinic, Acibadem Altunizade Hospital, Istanbul, Turkey, 2022

Breast Imaging Clinic, Acibadem Altunizade Hospital, Istanbul, Turkey, 2022

Breast Imaging Clinic, Acibadem Altunizade Hospital, Istanbul, Turkey, 2022
Figure 4

Breast Imaging Clinic, Acibadem Altunizade Hospital, Istanbul, Turkey, 2022