Clinical History
The patient presented with metatarsalgia, especially at weight bearing. There was no history of trauma.
Imaging Findings
The patient presented with metatarsalgia lasting for one month. The pain was more relevant at weight bearing. There was no history of direct trauma. The patient's investigation was negative for any bone metabolic disease.
The patient underwent X-ray that showed a fracture of the second metatarsal bone; she was treated with partial weight bearing.
After 2 months, due to the persistence of pain, the patient underwent a CT examination which confirmed the presence of the second metatarsal bone fracture and it also showed the presence of a fracture within the third metatarsal bone. A bone metabolism investigation was performed (negative).
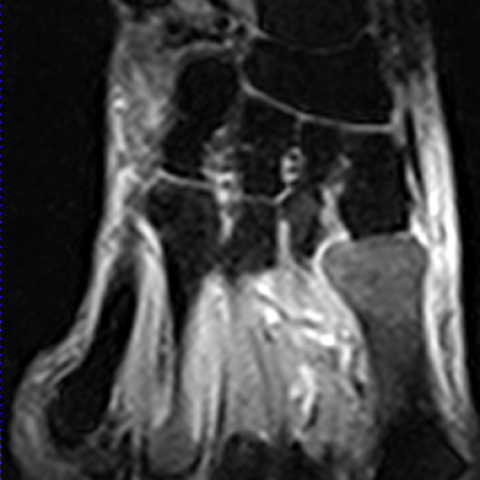
A MRI examination was performed (about one month later) in order to study soft tissues of the foot and bone marrow of the metatarsal bones. SE T1 confirmed the presence of the two fracture lines and STIR showed areas of bone marrow oedema within the proximal portion of the shaft of the first and second metatarsals, within the distal portion of the shaft of the third metatarsal bone and within the head of the fourth metatarsal bone. Moreover there was diffuse oedema of soft tissues.
These clinical, X-Ray, CT and MR features were compatible with SEQUENTIAL stress fractures (unusual presentation for multiple stress fractures, which normally occur together).
No therapy was recommended (only oral FANS to relieve the pain).
Discussion
Stress fractures occur in normal or metabolically weakened bones. They are classified into two groups: those that result from prolonged cyclical mechanical stress on normal bone are called "fatigue fractures", while those that occur with physiologic stress on bones weakened by metabolic disease or radiation treatment are called "insufficiency fractures". Incidence of fatigue fractures is increasing in the population, with runners now the most commonly affected group, accounting for 72% of stress fractures. Insufficiency fractures occur more commonly in the elderly and, in particular, in oncology patients.
Among the metatarsal bones, stress fractures involving the middle and distal portions of the shaft of the second and third metatarsals are most common. Stress fractures at the base of the first or second metatarsals or affecting other metatarsal bones are less common.
The pathogenesis of stress fractures is due to a cyclic, repetitive and submaximal loading of the bone. This creates numerous microfractures especially when the duration, intensity or frequency of physical activity is rapidly increased. If this damage is not abated through adequate rest, it ultimately exceeds the reparative ability of the skeletal system and the microfractures coalesce into a stress fracture.
Running is reported to be the predominant cause of stress fractures but other factors contribute to their development such as bone composition, vascular supply, hormonal imbalances, nutritional status and inappropriate footwear.
Most stress fractures are classified as low risk. Typically, the patient experiences an insidious onset of localised pain. Some stress fractures are classified as high risk. They manifest with vague pain and can lead to a prolonged recovery because of complications with bone union.
Radiography is the first line of diagnosis. The initial appearance may be normal but in other cases the classic feature is of a lucent fracture line associated with sclerosis, benign periosteal reaction and endosteal cortical thickening.
In CT the typical appearance of a stress fracture is that of focal callus formation and endosteal thickening around a fracture site. A helpful sign for distinguishing stress fractures from pathologic fractures is the presence of an aggressive periosteal reaction.
MRI findings include decreased marrow signal on T1 sequences and increased marrow signal on T2 sequences around a fracture line. The most sensitive discriminating feature between stress and pathologic fractures is a well-defined low signal T1 weighted abnormality around a fracture indicating an underlying tumour. For a whole-body approach, bone scans and PET scans carry an advantage over CT and MRI but they are nonspecific. In the evaluation of stress injuries, a bone scan can reveal changes before radiography but offers lower resolution and specificity to differentiate stress and pathologic fractures.
Similarly, PET scans may show FDG uptake at the site of a stress fracture, potentially mistaking the presence of a metastatic focus.
Low-risk stress fractures generally are easy to recognise and are treated with 6–8 weeks of relative rest. For high-risk stress fractures an aggressive treatment is warranted and it should be the surgical reduction of the fracture followed by 6–8 weeks of postoperative immobilisation.
Differential Diagnosis List
Sequential stress fractures of the metatarsal bones
Final Diagnosis
Sequential stress fractures of the metatarsal bones